Social Ecologist ‘at large’
http://mildgreens.blogspot.com/
http://blairformayor.blogspot.com/
http://blair4mayor.com/
ph (643) 389 4065 cell 027 265 7219
| There is inadequate evidence that cannabis, at the amount typically. consumed by pregnant women, causes low birth weight |
benzo.org.uk – Prescribed drugs do more harm to babies than heroin …
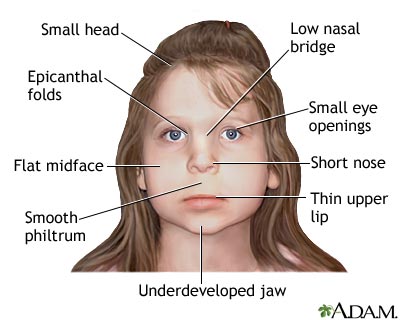
learn.sdstate.edu/nursing/FAS.html
In simplest terms, FAS is caused by prenatal exposure to “high” amounts of alcohol. The determination of “how much is too much” turns out to be a sticky problem. Diagnostic criteria refer to “maladaptive patterns of drinking associated with moderate to heavy alcohol consumption,” and in the extreme this is not particularly difficult to identify with reasonable certainty. However, defining limits for moderate amounts of alcohol is difficult, and the resulting potentially adverse effects cannot be excluded nor definitively demonstrated. In 1996, the Institute of Medicine (IOM) of the National Academy of Sciences published the findings of a committee that was formed to conduct a literature study of fetal alcohol syndrome and related birth defects, and to provide guidance for future research and prevention efforts (3). According to the IOM committee, “The lack of diagnostic criteria for or more definitive statements regarding possible effects of low to moderate exposure to alcohol should not be interpreted as contradictory to the Surgeon General’s warning against drinking alcohol during pregnancy.”
Previous to the IOM report, the term Fetal Alcohol Effects (FAE) was used to describe children who have all of the diagnostic features of FAS, but at mild or less severe levels. In the IOM report the terms ARND and ARBD were recommended, and are currently preferred.
The IOM report notes that ARBD and ARND are “catch-all” categories, and the outcomes are not specific to prenatal alcohol consumption. Thus, the causal link between maternal alcohol consumption and ARBD or ARND generally is not certain, and the role of other factors may need to be excluded. Both ARBD and ARND also require documented maternal alcohol exposure, and include outcomes linked to maternal alcohol consumption through human or animal research.
Alcohol-Related Birth Defects (ARBD) includes a diverse array of physical birth defects: skeletal abnormalities, heart defects, cleft palate and other craniofacial abnormalities, kidney and other internal organ problems, vision and hearing problem.
Alcohol-Related Neurodevelopmental Disorders (ARND) includes outcomes such as decreased cranial size at birth, structural brain abnormalities (e.g., microcephaly), abnormal neurological conditions ( e.g., impaired fine motor skills, neurosensory hearing loss, poor tandem gait, and poor eye-hand coordination). The IOM report also includes a diagnosis of ARND as a result of behavior or cognitive abnormalities that cannot be explained by other familial or environmental factors, and of course there is a history of maternal alcohol consumption.
Examples of behavior and cognitive abnormalities include:
- Learning difficulties
- Deficits in school performance
- Poor impulse control
- Problems in social perception
- Deficits in higher level receptive and expressive language
- Poor capacity for abstraction and metacognition
- Specific deficits in mathematical skills
- Problems in memory, attention, or judgement
References
1. Lemoine et al., Ouest Medecine 21, 476-482, 1968.
2. Jones, et al. Lancet 1, 1267-1271, 1973.
3. Institute of Medicine, Fetal Alcohol Syndrome: Diagnosis, Epidemiology, Prevention, and Treatment, Stratton, K., Howe, C., and Battaglia, F, Editors. National Academy Press, 1996.Defining Excessive Alcohol Consumption
Major Points to Remember:
- FAS is clearly associated with alcohol dependence and abuse
- Alcohol dependence and abuse are characterized by maladaptive patterns of drinking
- Alcohol consumption that results in dependence is considered a diagnosable disease
